20-Apr-2023
The Robotein® facility, which is part of Instruct-BE, offers biomolecular analysis and protein production under the umbrella of two academic laboratories in Belgium: the Centre for Protein Engineering (CIP) at the Université de Liège and the Structural Biology and Bioinformatics Centre at the Université Libre de Bruxelles. As part of a collaboration between various laboratories, and with significant input from Robotein®, four recent studies have explored in detail the effects and efficacy of the SARS-CoV-2 vaccine on specific demographics: nursing home residents, younger children, and kidney transplant recipients.
The studies, which have all taken place in the past 18 months, explore the impact of the SARS-CoV-2 BNT162b2 mRNA vaccine, and the extent to which breakthrough infection (BTI) has occurred within each group, and the structural basis for this BTI to happen.
One such study, from Tomasi et al, (2022) investigated the effect of the vaccine on young children (14 and under), finding that in a sample size of 48 individuals, serum titers showed high levels of IgG and IgA antibodies to S, S1 and the RBD of SARS-CoV-2, but not to S2. The study also illustrated a significant increase in the titres of IgG and IgA in children compared to adult sera, and that antibody titres remain similar between asymptomatic, mild, and hospitalised cases.
Another study from the labs (Pannus et al, 2022) analysed residents in nursing homes, using staff members in nursing homes as a control. This created four distinct groups: infection-naïve residents, infection-naïve staff, previously infected residents, and previously infected staff. Following the two mRNA vaccine doses, both antibody titres and avidity were found to be lower for infection-naïve residents compared to infection-naïve staff. By contrast, high antibody responses were observed for infected residents, with no significative difference with previously infected staff antibody responses.
Antibody avidity demonstrated differences between residents and staff. Particularly in the infection-naïve group, 49 days after primary vaccination, staff members had “markedly higher” levels of neutralising antibodies than residents. Even more significantly, the study examined the response to the B.1.351 variant, and found that none of the infection-naïve residents had detectable levels of neutralising antibodies to the particular strain – although it is notable that only 10% of infection-naïve staff had these antibodies.
In addition, analyses were also performed following the third mRNA vaccine dose (Pannus et al, 2023), which indicated strong antibody responses after the third dose for infection-naïve residents, similar to the infection-naïve staff. This observation suggested that the third dose might provide optimal protection for this vulnerable group.
In another recent study, Kemlin et al (2023) investigated the prevalence of BTI on transplant patients. Due to immunosuppressive therapies and susceptibility to secondary morbidities, solid organ transplant (SOT) recipients were given priority vaccination to COVID-19. However, it had been previously found that their response to two doses of the mRNA vaccine was weaker than healthy adults, with neutralising antibodies undetectable in many patients.
The third dose of the vaccine (booster) was found to be particularly important for these patients, with RBD-binding IgG increase by more than 4-fold between the second and third dose. Neutralising antibodies also increased, only detectable in 2% of patients after the second dose, and 45% of patients after the third.
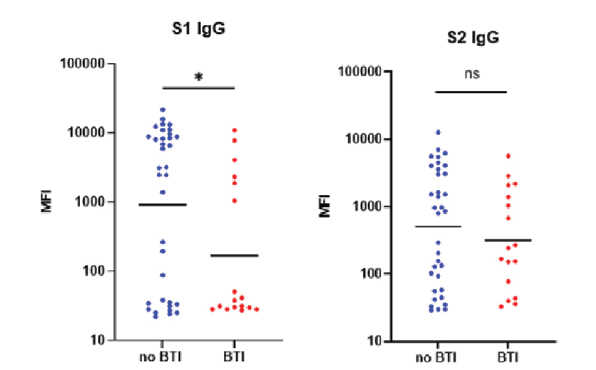
Figure 1. Difference in S1 and S2-binding antibodies between no BTI and BTI affected SOT patients. S1 binding is lower in BTI patients, however there is minimal difference between BTI and no-BTI patients for S2-binding antibodies.
Patients who experienced BTI were found to have much lower levels of S1-binding IgG antibodies (Figure 1). However, as found in previous studies, there was no difference in the levels of S2-binding antibodies between BTI patients and those without BTI. Similar to S1-binding, RBD-binding antibodies were higher in no-BTI patients. This further emphasises the importance of S1 and RBD-binding antibodies in vaccine development.
Biomolecular analysis conducted at Robotein® helped to conduct the biomolecular analysis of antibodies expressed in patient sera in combination with the viral proteins for the study. The four studies provide more insight into the efficacy and impact of vaccinations for various groups, and provide a platform for deeper understanding of which groups require priority for vaccination.
Find out more about the Robotein® facility here.
